
Multimedia Journal of Metaverse in MEDICINE
METHODOLOGY | JANUARY 2, 2025
Introduction to the “Nasal String” Internal Fixation Technique
Xiaoyun Kang¹, Nan Hao¹, Ruihua Li¹, Ting Li¹, Baiya Li², Yong Zhang¹*
1 Department of Surgical Oncology, The First Affiliated Hospital of Xi’an JiaoTong University, Xi’an 710061, China.
2 Department of Otorhinolaryngology, Head and Neck Surgery, Xi’an 710061, China.
Corresponding Authors: Yong Zhang. E-mail: [email protected]
Address: Department of Surgical Oncology, The First Affiliated Hospital of Xi’an JiaoTong University, Xi’an 710061, China.
Summary
The “Nasal String” internal fixation technique was clinically applied in 408 patients with significant success. Compared to the traditional external fixation method using dual nasogastric tubes, this technique significantly reduced the incidence of unintentional tube removal and fixation-related complications, while greatly improving patient comfort.
Abstract
This study compared the traditional external fixation method of dual nasogastric tubes with the “Nasal String” internal fixation technique in terms of unintentional tube removal, complication rates, and patient comfort. The results showed that the latter method was superior, suggesting that the “Nasal String” internal fixation method should be widely recommended.
Keywords
“Nasal String” internal fixation; dual nasogastric tubes; unplanned tube removal
Introduction
Esophageal and cardia cancers are common gastrointestinal tumors, and their incidence has been trending younger in recent years. Surgical treatment is the preferred approach. Preoperative placement of nasogastric and nasoenteric tubes is routine. However, traditional fixation methods are associated with an unintentional tube removal rate exceeding 20%, significantly hindering patient recovery and increasing both physical and mental discomfort. Foreign studies have reported the use of a flexible and firm material looped around the nasal septum, through one nostril and out the other, to secure the nasoenteric tube, with widespread clinical adoption. This article introduces a novel “nasal loop” dual-tube fixation technique aimed at benefiting more patients and conserving healthcare resources.
Protocol
The study protocol was reviewed and approved by the Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University in accordance with the ethical guidelines established by the Declaration of Helsinki. Patient safety and well-being are our primary concerns, and all procedures aim to minimize potential risks and discomfort. Collected data will remain confidential and be used solely for research purposes. Patients may withdraw from the study at any time without affecting their relationship with the researchers or institution.
1. General Information
Patients diagnosed with esophageal or cardia cancer requiring surgical treatment were included. A total of 405 patients who underwent surgery with nasogastric and feeding tube placement between July 2022 and July 2023 formed the observation group. From August 2023 to August 2024, 408 patients were included as study subjects after consenting to participate.
2. Inclusion and Exclusion Criteria:
(1) Inclusion Criteria:Patients range from ages 18-80 and are in stable condition without cognitive impairment;Confirmed diagnosis of esophageal or cardia cancer requiring surgical treatment;Suitable for nasogastric and feeding tube fixation;Informed consent obtained from the patient or guardian.
(2) Exclusion Criteria:History of traumatic brain injury;History of Oral or nasal surgery;Limited mouth opening;Uncooperative behavior;Cognitive impairment;Unstable condition.
3. Methods
(1) Traditional Fixation Method:
a. No contraindications for tube placement.
b. Disinfection of the nasal mucosa.
c. Lubrication of the catheter.
d. Standard insertion of nasogastric and feeding tubes.
e. 3M elastic adhesive tape was used to secure both the nasogastric and nasoenteric tubes in an “I” configuration on the patient’s nasal bridge, or in a “H” configuration to secure the face, both employing the elevated platform method.
(2) “Nasal String” Internal Fixation Method
a. No contraindications for tube placement.
b. Disinfect the nasal mucosa.
c. Insert two neonatal size 5 gastric tubes through the nostrils to a depth of 15-20cm.
d. Ask the patient to open their mouth widely to expose the oral pharynx.
e. Use a sterile hemostatic forcep to gently grasp both gastric tubes and pull them out through the mouth.
f. Using a sterile scissors, trim the tips of the gastric tubes to create a hollow lumen. Insert a surgical suture approximately 15 cm into the tips of each tube.
g. Pull the ends of the size 5 gastric tubes so that the surgical sutures form an inverted “V” shape, hanging on the nasal septum.
h. At 0.5cm outside of the nasal cavity, tie a knot using the surgical sutures to create a loop that wraps around the nasal septum.
i. Secure the feeding tube and gastric tube in place with the sutures.
Methods Video
REPRESENTATIVE RESULTS
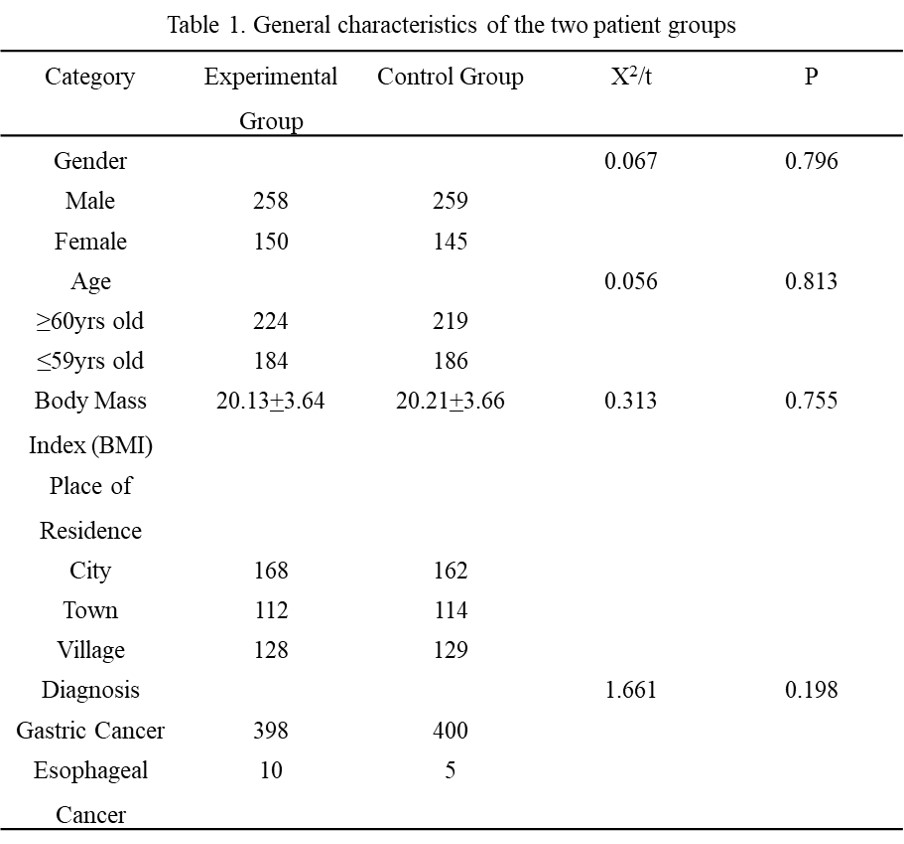
In this study, there were no statistically significant differences in the general information of patients between the experimental group and the control group (P > 0.05), as detailed in Table 1.
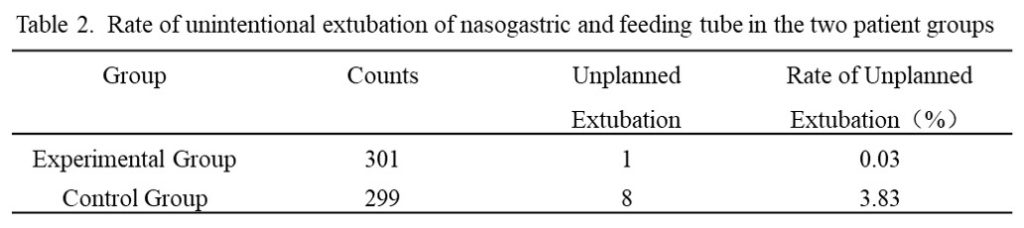
The incidence of unplanned tube removal was significantly lower in the experimental group compared to the control group (P < 0.001), as shown in Table 2.
Discussion
The “Nasal String” internal fixation technique was successfully applied in 408 patients without significant complications. This method notably reduced unintentional tube removal, improved patient comfort, and is suitable for clinical promotion. However, during application, attention should be focused on skin issues around the nasal area. It is recommended to check the nasal mucosa daily for signs of pressure, and to rotate the nasal string appropriately to reduce skin shearing pressure.
Conclusion
The development and clinical application of this technique were made possible by the joint efforts of all medical staff in the department and the cooperation of patients. Thank you all for your contributions.
Author Contributions
Xiaoyun Kang wrote the first draft. Nan Hao, Ruihua Li, Ting Li and Baiya Li contributed to the critical revision of the manuscript. Yong Zhang reviewed and revised the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
None.
Conflicts of Interest
The authors declare no conflict of interest.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Received: 14 November 2024
Accepted: 17 December 2024
Published on line: 2 January 2025
Reference
- McGuirt WF, Strout JJ. “How I do it”–head and neck. A targeted problem and its solution: securing of intermediate duration feeding tubes. Laryngoscope. 1980, 90(12):2046-8.
- Popovich MJ, Lockrem JD, Zivot JB. Nasal bridle revisited: an improvement in the technique to prevent unintentional removal of small-bore nasoenteric feeding tubes. Crit Care Med. 1996, 24(3):429-31.
- Soria A, Santacruz E, Vega-Piñeiro B, Gión M, Molina J, Villamayor M, Mateo R, Riveiro J, Nattero L, Botella-Carretero JI. Gastrostomy vs nasogastric tube feeding in patients with head and neck cancer during radiotherapy alone or combined chemoradiotherapy. Nutr Hosp. 2017, 34(3):512-516.
- Inayat F, Ur Rahman A, Almas T, Zahid E, Zervos X. Nasal Bridles for Securing Nasoenteric Feeding Tubes: A Review of Clinical Effectiveness and Potential Complications. Cureus. 2020, 12(5): e8325.
- Gunn SR, Early BJ, Zenati MS, Ochoa JB. Use of a nasal bridle prevents accidental nasoenteral feeding tube removal. JPEN J Parenter Enteral Nutr. 2009, 33(1):50-4.
- Lewis SJ, Egger M, Sylvester PA, Thomas S. Early enteral feeding versus “nil by mouth” after gastrointestinal surgery: systematic review and meta-analysis of controlled trials. BMJ. 2001, 323(7316):773-6.
- Seder CW, Stockdale W, Hale L, Janczyk RJ. Nasal bridling decreases feeding tube dislodgment and may increase caloric intake in the surgical intensive care unit: a randomized, controlled trial. Crit Care Med. 2010, 38(3):797-801.
- Popovich MJ, Lockrem JD, Zivot JB. Nasal bridle revisited: an improvement in the technique to prevent unintentional removal of small-bore nasoenteric feeding tubes. Crit Care Med. 1996, 24(3):429-31.
- Bechtold ML, Nguyen DL, Palmer LB, Kiraly LN, Martindale RG, McClave SA. Nasal bridles for securing nasoenteric tubes: a meta-analysis. Nutr Clin Pract. 2014, 29(5):667-71.
- Parks J, Klaus S, Staggs V, Pena M. Outcomes of nasal bridling to secure enteral tubes in burn patients. Am J Crit Care. 2013, 22(2):136-42.
- Beavan J, Conroy SP, Harwood R, Gladman JR, Leonardi-Bee J, Sach T, Bowling T, Sunman W, Gaynor C. Does looped nasogastric tube feeding improve nutritional delivery for patients with dysphagia after acute stroke? A randomised controlled trial. Age Ageing. 2010, 39(5):624-30.
- Flores-Verastegui MIM, Coe S, Tammam J, Almahjoubi H, Bridle R, Bi S, Thondre PS. Effects of Frozen Red Dragon Fruit Consumption on Metabolic Markers in Healthy Subjects and Individuals at Risk of Type 2 Diabetes. Nutrients. 2025, 17(3):441.
- Webb G, Gupta P, Fitchett J, Simmons J, De Silva A. Efficacy of nasal bridles in avoiding percutaneous endoscopic gastrostomy placement. Frontline Gastroenterol. 2012, 3(2):109-111.
- Johnston RD, O’Dell L, Patrick M, Cole AT, Cunliffe RN. Outcome of patients fed via a nasogastric tube retained with a bridle loop: do bridle loops reduce the requirement for percutaneous endoscopic gastrostomy insertion and 30-day mortality? Proc Nutr Soc. 2008, 67(OCE3): E116.
- Li AY, Rustad KC, Long C, Rivera E, Mendiola M, Schenone M, Karanas YL. Reduced incidence of feeding tube dislodgement and missed feeds in burn patients with nasal bridle securement. Burns. 2018, 44(5):1203-1209.
- Brugnolli A, Ambrosi E, Canzan F, Saiani L; Naso-gastric Tube Group. Securing of naso-gastric tubes in adult patients: a review. Int J Nurs Stud. 2014, 51(6):943-50.
- Lynch A, Tang CS, Jeganathan LS, Rockey JG. A systematic review of the effectiveness and complications of using nasal bridles to secure nasoenteral feeding tubes. Aust J Otolaryngol. 2018, 1:8.
- Jackson RS, Sharma S. Retained nasal tube bridle system insertion stylet presenting as nasal foreign body: a report of two cases. Am J Otolaryngol. 2015, 36(2):296-8.
- Smith C, Saravanapavan H, Mann S. An unusual complication of a nasogastric retaining device: a case study. Gastrointest Nurs. 2016, 14:25–27.
- Puricelli MD, Newberry CI, Gov-Ari E. Avulsed Nasoenteric Bridle System Magnet as an Intranasal Foreign Body. Nutr Clin Pract. 2016, 31(1):121-4.