
Multimedia Journal of Metaverse in MEDICINE
METHODOLOGY | JANUARY 2, 2025
Application of Pulmonary Three-Dimensional Reconstruction in Surgeryue
Ruoxi Zhong¹, CHAN FAY FEI YI¹, Qiong Wang¹, Yong Zhang¹*
1 Department of Surgical Oncology, The First Affiliated Hospital of Xi’an JiaoTong University, Xi’an 710061, China.
2 Department of Otorhinolaryngology, Head and Neck Surgery, Xi’an 710061, China.
Corresponding Authors: Yong Zhang. E-mail: [email protected]
Address: Department of Surgical Oncology, The First Affiliated Hospital of Xi’an JiaoTong University, Xi’an 710061, China.
Summary
Existing studies have demonstrated that the application of pulmonary three-dimensional (3D) reconstruction technology in clinical surgery provides significant guidance for the intraoperative localization of pulmonary nodules. Compared with the standard group, the reconstruction group has a shorter average surgical time for nodule identification, especially when the lesion is in deep and complex segments.
Abstract
This case utilized pulmonary 3D reconstruction technology for the auxiliary localization and identification of a nodule. The nodule in the outer basal segment of the left lower lobe was clearly displayed, allowing for dynamic rotation and measurement operations to accurately determine the lesion’s location.
Keywords
three-dimensional; nodule; auxiliary localization
Introduction
With the increasing precision and diversification of diagnostic methods, more and more patients with early-stage lung cancer are being detected. Surgical resection remains the primary treatment for lung cancer, and the number of minimally invasive surgeries has increased significantly in recent years, gradually being widely adopted and achieving remarkable outcomes. Segmentectomy for early-stage lung cancer can achieve good long-term prognosis, maximizing the removal of the lesion while preserving the function of normal lung tissue. This requires surgeons to have a clear understanding of the location of the lesion, its adjacent structures, and the branching patterns of the target lobe, segment, bronchi, and blood vessels. Pulmonary three-dimensional (3D) reconstruction technology can effectively assist in this process, providing a more intuitive display of vascular branching patterns and anatomical variations of blood vessels and bronchi. It also helps in delineating the extent of the lesion, preoperative localization, surgical planning, preoperative simulation, and intraoperative navigation, playing a positive role in individualized anatomical segmentectomy.
Protocol
The patient underwent thin-slice contrast-enhanced CT scanning. The imaging data were recorded onto a CD, and the DICOM-format images were imported into the reconstruction software. Manual annotation and identification were performed to complete the reconstruction. Initially, the starting points of each segmental pulmonary artery are manually identified. Subsequently, the computer automatically segments the lungs based on the pulmonary artery distribution and further divides them into subsegments according to the subsegmental pulmonary artery origins. The process primarily relies on the seed line method, with manual extraction serving as a supplementary approach. The lung parenchyma is maximally extracted and integrated with the segmented divisions to generate corresponding modules and assign distinct colors. Next, the CT images are adjusted to the pulmonary artery window, and the entire arterial tree is segmented using the seed point method. The same technique is applied to delineate the venous vascular tree. The bronchial reconstruction is then completed by adjusting the threshold to the bronchial range and using a combination of threshold segmentation and the seed point method. Finally, pulmonary nodules are segmented and reconstructed. Larger nodules are extracted using the threshold and seed point methods, while smaller nodules are manually delineated. By combining the 3D images of the pulmonary nodules with the 3D lung images and adjusting the transparency of the lung images, the precise location of the nodules and their corresponding pulmonary segment or subsegment can be clearly visualized.
Methods Video
The reconstructions of trachea and bronchi, pulmonary lesion, pulmonary vessels and lung are shown in Figure 1. The 3D reconstruction model is shown in Video. Please scan this QR code to watch the methods video.
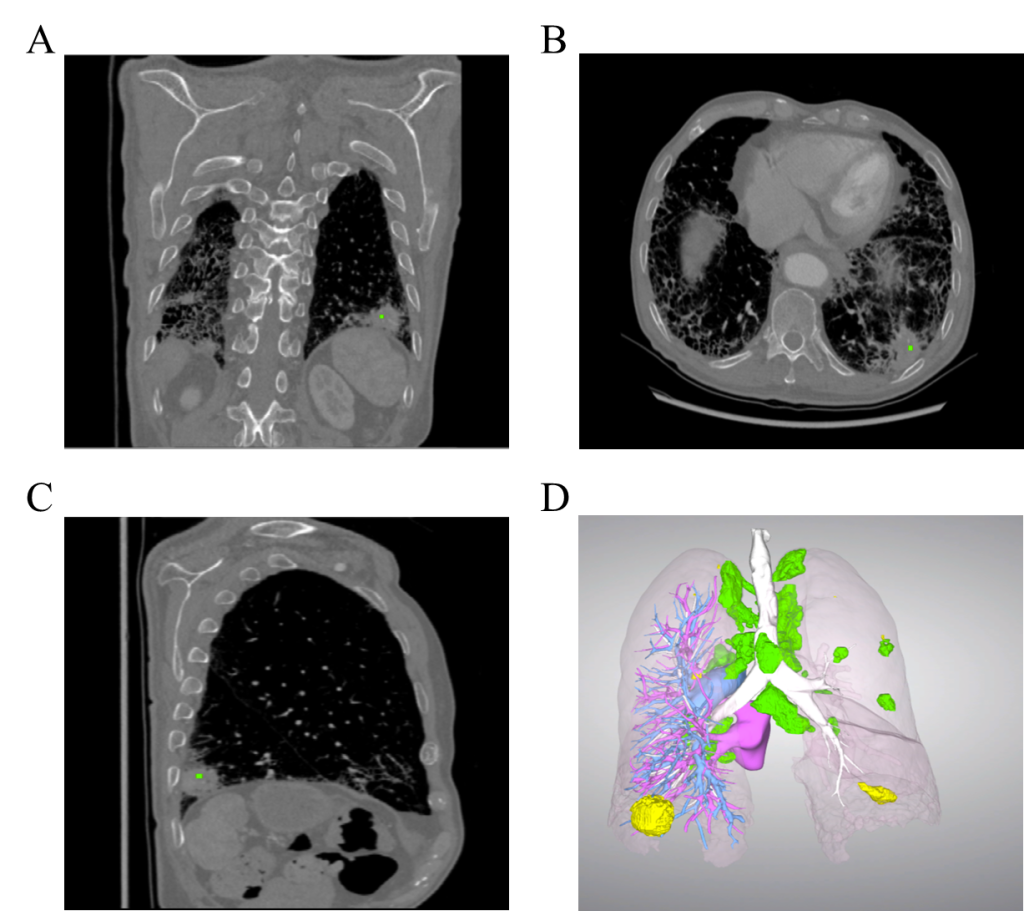
Fig.1 Patient’s thin-layer enhanced CT scan image and three-dimensional lung reconstruction image.
(A-C: Patient’s thin-layer enhanced CT scan image; D: the pulmonary artery is shown in blue, the pulmonary vein in purple, the trachea and bronchi in white, the nodule in the lower lobe of the left lung in yellow, and the lymph nodes in green).
REPRESENTATIVE RESULTS
This case involves a 69-year-old male (medical history information). Contrast-enhanced CT revealed an irregular mass in the outer basal segment of the left lower lobe, measuring approximately 29×28 mm, with a lobulated appearance and spiculation. There was also pleural traction adjacent to the mass, and the enhanced scan showed marked heterogeneous enhancement. The diagnosis was peripheral lung cancer in the outer basal segment of the left lower lobe.
Discussion
Pulmonary three-dimensional (3D) reconstruction technology is highly compatible with segmentectomy, providing a convenient, anatomically precise, and user-friendly individualized guidance for surgical procedures. The integration of this technology simplifies surgical operations, clarifies anatomical structures, and enhances the overall efficiency of the procedure. Promoting the application of pulmonary 3D reconstruction technology in future surgeries is expected to yield significant benefits with minimal effort, thereby improving surgical outcomes and patient care.
Conclusion
In conclusion, pulmonary three-dimensional (3D) reconstruction technology serves as a valuable tool for preoperative planning and intraoperative navigation in anatomical segmentectomy, particularly for lesions located in deep or complex pulmonary segments. This case demonstrated its efficacy in precisely localizing a nodule in the outer basal segment of the left lower lobe, enabling dynamic visualization of anatomical structures and optimized surgical workflow. By integrating vascular, bronchial, and parenchymal reconstructions, the technology enhances surgical precision, reduces operative time, and minimizes damage to healthy lung tissue. Its ability to clarify anatomical variations and guide individualized resection strategies underscores its clinical significance.
Author Contributions
Ruoxi Zhong wrote the first draft. CHAN FAY FEI YI and Qiong Wang contributed to the critical revision of the manuscript. Yong Zhang reviewed and revised the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
None.
Conflicts of Interest
The authors declare no conflict of interest.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Received: 14 October 2024
Accepted: 5 December 2024
Published on line: 2 January 2025
Reference
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021,71(3):209-249.
- Allemani C, Matsuda T, Di Carlo V, et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. 2018,391(10125):1023-1075.
- Wu Z, Huang Z, Qin Y, Jiao W. Progress in three-dimensional computed tomography reconstruction in anatomic pulmonary segmentectomy. Thorac Cancer. 2022,13(13):1881-1887.
- Natale G, Leonardi B, Messina G, et al. Three-dimensional lung reconstructions for the localization of lung nodules to be resected during surgery. Thorac Cancer. 2023,14(34):3389-3396.
- Chan EG, Landreneau JR, Schuchert MJ, et al. Preoperative (3-dimensional) computed tomography lung reconstruction before anatomic segmentectomy or lobectomy for stage I non-small cell lung cancer. J Thorac Cardiovasc Surg. 2015,150(3):523-528.
- Laven IEWG, Oosterhoff VPS, Franssen AJPM, et al. Evaluating three-dimensional lung reconstructions for thoracoscopic lung resections using open-source software: a pilot study. Transl Lung Cancer Res. 2024,13(7):1595-1608.
- Rui W, Yuhang S, Yang L, et al. A new method for evaluating lung volume: AI-3D reconstruction. Front Physiol. 2023,14:1217411.